|
Laryngeal Cancer
 Cancer of the larynx (or voicebox) is a disease in which malignant cells are
found in the tissues of the larynx. The larynx is a short passageway shaped like
a triangle that is just below the pharynx in the neck. The pharynx is a hollow
tube about 5 inches long that starts behind the nose and goes down to the neck
to become part of the oesophagus, the tube that goes to the stomach. Air passes
through the pharynx and then the larynx on the way to the windpipe (trachea) and
into the lungs. Food passes through the pharynx on the way to the oesophagus.
The larynx has a small piece of tissue over it, called the epiglottis, to keep
food from going into it or the air passages. Cancer of the larynx (or voicebox) is a disease in which malignant cells are
found in the tissues of the larynx. The larynx is a short passageway shaped like
a triangle that is just below the pharynx in the neck. The pharynx is a hollow
tube about 5 inches long that starts behind the nose and goes down to the neck
to become part of the oesophagus, the tube that goes to the stomach. Air passes
through the pharynx and then the larynx on the way to the windpipe (trachea) and
into the lungs. Food passes through the pharynx on the way to the oesophagus.
The larynx has a small piece of tissue over it, called the epiglottis, to keep
food from going into it or the air passages.
The larynx contains the vocal cords, which vibrate and make sound when air is
directed against them. The sound echoes through the pharynx, mouth, and nose to
make a person’s voice. The muscles in the pharynx, face, tongue, and lips help
people form words with sounds to make them understandable.
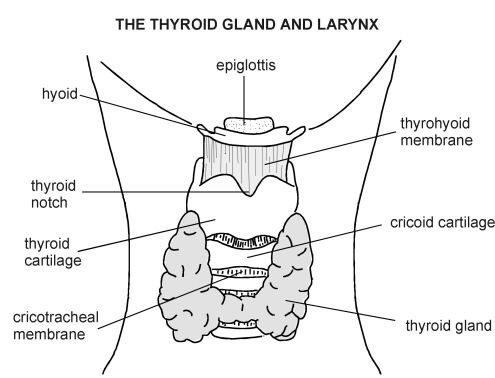
There are three main parts of the larynx:
- The glottis (the middle part of the larynx where the vocal
cords are)
- The supraglottis (the tissue above the glottis)
- The subglottis (the tissue below the glottis). The subglottis
connects to the trachea, which takes air to the lungs.
Cancer of the larynx is most commonly found in people who smoke. If a person
has cancer of the larynx and smokes, smoking should be stopped.
A doctor should be seen if the following symptoms appear:
- A sore throat that does not go away
- Pain when swallowing
- A change or hoarseness in the voice
- Pain in the ear
- A lump in the neck
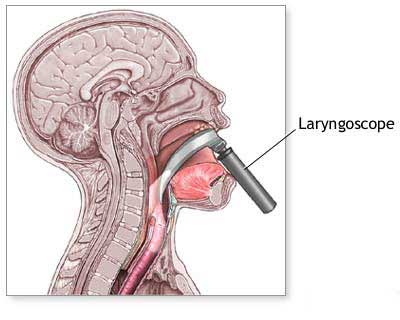
If there are symptoms, a doctor will put a tube with a special light on the
end of it down the patient’s throat to look at the larynx. This is called
laryngoscopy. If tissue that is not normal is found, the doctor will need to cut
out a small piece and look at it under the microscope to see if there are any
cancer cells. This is called a biopsy. The doctor will also feel the throat for
lumps.
 The chance of recovery (prognosis) depends on where the cancer is in the
larynx, whether the cancer is just in the larynx or has spread to other tissues
(the stage), and the patient’s general state of health. The chance of recovery (prognosis) depends on where the cancer is in the
larynx, whether the cancer is just in the larynx or has spread to other tissues
(the stage), and the patient’s general state of health.
Stages of cancer of the larynx
Once cancer of the larynx is found, more tests will be done to find out if
cancer cells have spread to other parts of the body. This is called staging. A
doctor needs to know the stage of the disease to plan treatment. In cancer of
the larynx, the definitions of the early stages depend on where the cancer
started. The following stages are used for cancer of the larynx:
Stage I
The cancer is only in the area where it started and has not spread to lymph
nodes in the area or to other parts of the body (lymph nodes are small
bean-shaped structures that are found throughout the body; they produce and
store infection-fighting cells). The exact definition of stage I depends on
where the cancer started, as follows:
Supraglottis
The cancer is only in one area of the supraglottis and the vocal cords can
move normally.
Glottis
The cancer is only in the vocal cords and the vocal cords can move normally.
Subglottis
The cancer has not spread outside of the subglottis.
Stage II
The cancer is only in the larynx and has not spread to lymph nodes in the
area or to other parts of the body. The exact definition of stage II depends on
where the cancer started, as follows:
Supraglottis
The cancer is in more than one area of the supraglottis, but the vocal cords
can move normally.
Glottis
The cancer has spread to the supraglottis or the subglottis or both. The
vocal cords may or may not be able to move normally.
Subglottis
The cancer has spread to the vocal cords, which may or may not be able to
move normally.
Stage III
Either of the following may be true:
- The cancer has not spread outside of the larynx, but the vocal
cords cannot move normally, or the cancer has spread to tissues next to the
larynx.
- The cancer has spread to one lymph node on the same side of
the neck as the cancer, and the lymph node measures no more than 3 centimetres
(just over 1 inch).
Stage IV
Any of the following may be true:
- The cancer has spread to tissues around the larynx, such as
the pharynx or the tissues in the neck. The lymph nodes in the area may or may
not contain cancer.
- The cancer has spread to more than one lymph node on the same
side of the neck as the cancer, to lymph nodes on one or both sides of the
neck, or to any lymph node that measures more than 6 centimetres (over 2
inches).
- The cancer has spread to other parts of the body.
Recurrent
Recurrent disease means that the cancer has come back (recurred) after it has
been treated. It may come back in the larynx or in another part of the body.
How cancer of the larynx is treated
There are treatments for all patients with cancer of the larynx. Three kinds
of treatment are used:
- Radiation therapy (using high-dose x-rays or other high-energy
rays to kill cancer cells)
- Surgery (taking out the cancer)
- Chemotherapy (using drugs to kill cancer cells)
Radiation therapy uses high-energy x-rays to kill cancer cells and shrink
tumours. Radiation may come from a machine outside the body (external radiation
therapy) or from putting materials that produce radiation (radioisotopes)
through thin plastic tubes in the area where the cancer cells are found
(internal radiation therapy). External radiation to the thyroid or the pituitary
gland may change the way the thyroid gland works. The doctor may wish to test
the thyroid gland before and after therapy to make sure it is working properly.
Giving drugs with the radiation therapy to make the cancer cells more sensitive
to radiation (radiosensitization) is being tested in clinical trials. Radiation
given in several small doses per day (hyperfractionated radiation therapy) is
also being tested in clinical trials. If smoking is stopped before radiation
therapy is started, there is a better chance of surviving longer.
Surgery is a common treatment of cancer of the larynx. A doctor may remove
the cancer and part of the larynx using one of the following operations:
- A cordectomy takes out only the vocal cord.
- A supraglottic laryngectomy takes out only the supraglottis.
- A partial or hemilaryngectomy removes only part of the larynx.
- A total laryngectomy removes the entire larynx. During this
operation, a hole is made in the front of the neck to allow the patient to
breathe. This is called a tracheostomy. If cancer has spread to lymph nodes,
the lymph nodes will be removed (lymph node dissection).
- Laser surgery may be used for very early cancers of the
larynx. During laser surgery, a narrow, intense beam of light is used to cut
out the cancer.
Chemotherapy uses drugs to kill cancer cells. Chemotherapy may be taken by
pill, or it may be put into the body by a needle in a vein or muscle.
Chemotherapy is called a systemic treatment because the drug enters the
bloodstream, travels through the body, and can kill cancer cells throughout the
body.
People with larynx cancer have a higher risk of getting other cancers in the
head and neck area. Clinical trials of chemoprevention therapy are testing
whether certain drugs can prevent second cancers from developing in the mouth,
throat, windpipe, nose, or oesophagus (the tube that connects the throat to the
stomach).
Because the larynx helps with breathing and talking, a patient may need
special help adjusting to the side effects of the cancer and its treatment. A
patient may need to learn a new way of talking, or may need a special device to
help with talking. The patient’s doctor will consult with several kinds of
doctors who can help determine the best treatment. Trained medical staff can
also help the patient recover from treatment and adjust to new ways of eating
and talking.
Stage I Laryngeal Cancer
Treatment depends on where the cancer is found in the larynx.
If cancer is in the supraglottis, treatment may be one of the following:
- External beam radiation therapy
- Surgery to remove the supraglottis (supraglottic laryngectomy)
- Surgery to remove the larynx (total laryngectomy)
If the cancer is in the glottis, treatment may be one of the following:
- Radiation therapy
- Surgery to take out a vocal cord (cordectomy)
- Surgery to remove part of the larynx (hemilaryngectomy) or
total laryngectomy
- Laser surgery
If the cancer is in the subglottis, treatment will probably be radiation
therapy. In some cases, a hemilaryngectomy may be done.
Stage II Laryngeal Cancer
Treatment depends on where the cancer is found in the larynx.
If the cancer is in the supraglottis, treatment may be one of the following:
- External-beam radiation therapy
- Surgery to remove the supraglottis (supraglottic laryngectomy)
or the entire larynx (laryngectomy).
- Radiation therapy may be given after surgery.
- A clinical trial of several small doses of radiation per day (hyperfractionated
radiation therapy).
- A clinical trial of chemoprevention therapy to prevent a
second cancer in the mouth, throat, windpipe, nose, or oesophagus.
If the cancer is in the glottis, treatment may be one of the following:
- Radiation therapy.
- Surgery to remove part of the larynx (hemilaryngectomy) or
total laryngectomy.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy).
- A clinical trial of chemoprevention therapy to prevent a
second cancer in the mouth, throat, windpipe, nose, or oesophagus.
If the cancer is in the subglottis, treatment may be one of the following:
- Radiation therapy.
- Surgery to remove part of the larynx (hemilaryngectomy) or
total laryngectomy.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy).
- A clinical trial of chemoprevention therapy to prevent a
second cancer in the mouth, throat, windpipe, nose, or oesophagus.
Clinical trials are evaluating the use of several smaller doses of radiation
per day (hyperfractionated radiation therapy).
Stage III Laryngeal Cancer
Treatment depends on where the cancer is found in the larynx.
If the cancer is in the supraglottis, treatment may be one of the following:
- Surgery to remove the cancer with or without radiation
therapy.
- Radiation therapy. Surgery to remove the larynx (laryngectomy)
may be needed if the cancer does not shrink after radiation.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy)
- A clinical trial of chemotherapy followed by radiation therapy
or chemotherapy combined with radiation therapy. Surgery to remove the larynx
(laryngectomy) may be needed if the cancer does not shrink after chemotherapy
and radiation.
- Clinical trials of chemotherapy, the use of drugs to make the
cancer cells more sensitive to radiation (radiosensitizers), or new forms of
radiation.
- Chemoprevention therapy to prevent a second cancer in the
mouth, throat, windpipe, nose, or oesophagus.
If the cancer is in the glottis, treatment may be one of the following:
- Surgery with or without radiation therapy.
- Radiation therapy. Surgery to remove the larynx (laryngectomy)
may be needed if the cancer does not shrink after radiation.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy)
- A clinical trial of chemotherapy followed by radiation therapy
or chemotherapy combined with radiation therapy. Surgery to remove the larynx
(laryngectomy) may be needed if the cancer does not shrink after chemotherapy
and radiation.
- Clinical trials of chemotherapy, the use of drugs to make the
cancer cells more sensitive to radiation (radiosensitizers), or new forms of
radiation.
- Chemoprevention therapy to prevent a second cancer in the
mouth, throat, windpipe, nose, or oesophagus.
If the cancer is in the subglottis, treatment may be one of the following:
- Surgery to remove the larynx (total laryngectomy), some of the
tissue around it, the thyroid gland while preserving the parathyroid glands
located near the thyroid, and the lymph nodes in the neck. Surgery is usually
followed by radiation therapy.
- Radiation therapy if a patient cannot have surgery.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy)
- Clinical trials of chemotherapy, the use of drugs to make the
cancer cells more sensitive to radiation (radiosensitizers), or new forms of
radiation.
- Chemoprevention therapy to prevent a second cancer in the
mouth, throat, windpipe, nose, or oesophagus
Stage IV Laryngeal Cancer
Treatment depends on where the cancer is found in the larynx.
If the cancer is in the supraglottis, treatment may be one of the following:
- Surgery to remove the larynx (total laryngectomy) followed by
radiation therapy.
- Radiation therapy. Surgery to remove the larynx (laryngectomy)
may be needed if the cancer does not shrink after radiation.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy)
- A clinical trial of chemotherapy followed by radiation therapy
or chemotherapy combined with radiation therapy. Surgery to remove the larynx
(laryngectomy) may be needed if the cancer does not shrink after chemotherapy
and radiation.
- Clinical trials of chemotherapy, the use of drugs to make the
cancer cells more sensitive to radiation (radiosensitizers), or new forms of
radiation.
- Chemoprevention therapy to prevent a second cancer in the
mouth, throat, windpipe, nose, or oesophagus.
If the cancer is in the glottis, treatment may be one of the following:
- Total laryngectomy followed by radiation therapy.
- Radiation therapy. Surgery to remove the larynx (laryngectomy)
may be needed if the cancer does not shrink after radiation.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy)
- A clinical trial of chemotherapy followed by radiation therapy
or chemotherapy combined with radiation therapy. Surgery to remove the larynx
(laryngectomy) may be needed if the cancer does not shrink after chemotherapy
and radiation.
- Clinical trials of chemotherapy, the use of drugs to make the
cancer cells more sensitive to radiation (radiosensitizers), or new forms of
radiation.
- Chemoprevention therapy to prevent a second cancer in the
mouth, throat, windpipe, nose, or oesophagus.
If the cancer is in the subglottis, treatment may be one of the following:
- Total laryngectomy, removal of the thyroid gland, and removal
of some of the tissue around the larynx and the lymph nodes in the neck.
Surgery is usually followed by radiation therapy.
- Radiation therapy if a patient cannot have surgery. Clinical
trials are testing new ways of giving radiation therapy and the use of
radiosensitizers.
- A clinical trial of several smaller doses of radiation per day
(hyperfractionated radiation therapy)
- A clinical trial of chemotherapy and hyperfractionated
radiation therapy given at the same time.
- Clinical trials of chemotherapy, the use of drugs to make the
cancer cells more sensitive to radiation (radiosensitizers), or new forms of
radiation.
- Chemoprevention therapy to prevent a second cancer in the
mouth, throat, windpipe, nose, or oesophagus.
Recurrent Laryngeal Cancer
Treatment depends on the kind of treatment the patient had when first
treated. If the patient had surgery alone, the patient may have surgery again or
radiation therapy. If the patient had radiation therapy alone, additional
radiation therapy or surgery may be considered. If the patient failed surgery
and radiation therapy, clinical trials of chemotherapy may be given to relieve
symptoms.
BACK |
|
Lip and Oral Cavity Cancer
Cancer of the lip and oral cavity is a disease in which cancer cells are
found in the tissues of the lip or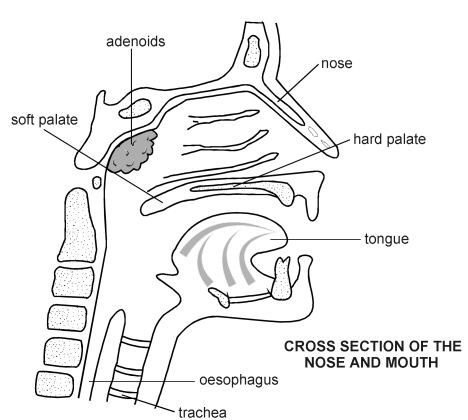 mouth. The oral cavity includes the front two
thirds of the tongue, the upper and lower gums (the gingiva), the lining of the
inside of the cheeks and lips (the buccal mucosa), the bottom (floor) of the
mouth under the tongue, the bony top of the mouth (the hard palate), and the
small area behind the wisdom teeth (the retromolar trigone). mouth. The oral cavity includes the front two
thirds of the tongue, the upper and lower gums (the gingiva), the lining of the
inside of the cheeks and lips (the buccal mucosa), the bottom (floor) of the
mouth under the tongue, the bony top of the mouth (the hard palate), and the
small area behind the wisdom teeth (the retromolar trigone).
Cancers of the head and neck are most often found in people who are over the
age of 45. Cancer of the lip is more common in men than in women, and is more
likely to develop in people with light-coloured skin who have been in the sun a
lot. Cancer of the oral cavity is more common in people who chew tobacco or
smoke pipes.
A doctor should be seen if a person finds a lump in the lip,
mouth, or gums, finds a sore in the mouth that doesn’t heal, or has bleeding or
pain in the mouth. Another sign of a cancer of the mouth or gums is when
dentures no longer fit well. Often lip and oral cavity cancers
 are
found by dentists when examining the teeth. are
found by dentists when examining the teeth.
If there are symptoms, a doctor will examine the mouth using a mirror and
lights. The doctor may order x-rays of the mouth. If tissue that is not normal
is found, the doctor will need to cut out a small piece and look at it under the
microscope to see if there are any cancer cells. This is called a biopsy. The
patient will be given a substance to take feeling away from the area for a short
time (a local anaesthetic) so no pain is felt. The doctor will also feel the
throat for lumps.
The chance of recovery (prognosis) depends on where the cancer is in the lip
or mouth, whether the cancer is just in the lip or mouth or has spread to other
tissues (the stage), and the patient’s general state of health.
Stage of cancer of the lip and oral cavity
 Once cancer of the lip and oral cavity is found, more tests will be done to
find out if cancer cells have spread to other parts of the body. This is called
staging. A doctor needs to know the stage of the disease to plan treatment. The
following stages are used for cancer of the lip and oral cavity: Once cancer of the lip and oral cavity is found, more tests will be done to
find out if cancer cells have spread to other parts of the body. This is called
staging. A doctor needs to know the stage of the disease to plan treatment. The
following stages are used for cancer of the lip and oral cavity:
Stage I
The cancer is no more than 2 centimetres (about 1 inch) and has not spread to
lymph nodes in the area (lymph nodes are small bean-shaped structures that are
found throughout the body; they produce and store infection-fighting cells).
Stage II
The cancer is more than 2 centimetres, but less than 4 centimetres (less than
2 inches), and has not spread to lymph nodes in the area.
Stage III
Either of the following may be true:
- The cancer is more than 4 centimetres.
- The cancer is any size but has spread to only one lymph node
on the same side of the neck as the cancer. The lymph node that contains
cancer measures no more than 3 centimetres (just over one inch).
Stage IV
Any of the following may be true:
- The cancer has spread to tissues around the lip and oral
cavity. The lymph nodes in the area may or may not contain cancer.
- The cancer is any size and has spread to more than one lymph
node on the same side of the neck as the cancer, to lymph nodes on one or both
sides of the neck, or to any lymph node that measures more than 6 centimetres
(over 2 inches).
- The cancer has spread to other parts of the body.
Recurrent
Recurrent disease means that the cancer has come back (recurred) after it has
been treated. It may come back in the lip and oral cavity or in another part of
the body.
How cancer of the lip and oral cavity is treated
There are treatments for all patients with cancer of the lip and oral cavity.
Two kinds of treatment are used:
- Surgery (taking out the cancer)
- Radiation therapy (using high-dose x-rays or other high-energy
rays to kill cancer cells)
Chemotherapy (using drugs to kill cancer cells) is being tested in clinical
trials.
Surgery is a common treatment of cancer of the lip and oral cavity. The
doctor may remove the cancer and some of the healthy tissue around the cancer.
The doctor may also remove the lymph nodes in the neck (lymph node dissection).
Radiation therapy uses high-energy x-rays to kill cancer cells and shrink
tumours. Radiation may come from a machine outside the body (external radiation
therapy) or from putting materials that produce radiation (radioisotopes)
through thin plastic tubes or needles in the area where the cancer cells are
found (internal radiation therapy). If smoking is stopped before radiation
therapy is started, the patient has a better chance of surviving longer.
Chemotherapy uses drugs to kill cancer cells. Chemotherapy may be taken by
pill, or it may be put into the body by a needle in a vein or muscle.
Chemotherapy is called a systemic treatment because the drug enters the
bloodstream, travels through the body, and can kill cancer cells throughout the
body.
If the doctor removes all the cancer that can be seen at the time of the
operation, the patient may be given chemotherapy after surgery to kill any
cancer cells that are left. Chemotherapy given after an operation to a person
who has no cancer cells that can be seen is called adjuvant chemotherapy.
Chemotherapy given before surgery to try and shrink the cancer so it can be
removed is called neoadjuvant chemotherapy.
Hyperthermia is a new treatment being tested in certain patients. It uses a
special machine to heat the body for a certain period of time to kill cancer
cells. Because cancer cells are often more sensitive to heat than normal cells,
the cancer cells die and the cancer shrinks.
Because the lips and mouth are needed to eat and talk, a patient may need
special help adjusting to the side effects of the cancer and its treatment. The
doctor will consult with several kinds of doctors who can help determine the
best treatment for the patient. Trained medical staff can also help a patient
recover from treatment and adjust to new ways of eating and talking. A patient
may need plastic surgery or help learning to eat and speak if a large part of
the lip or mouth is taken out.
Stage I Lip and Oral Cavity Cancer
Treatment depends on where the cancer is in the lip or mouth.
Lip cancer
If the cancer is in the lip, treatment may be one of the following:
- Surgery.
- Radiation therapy.
Tongue cancer
If the cancer is in the tongue, treatment may be one of the following:
- Surgery.
- Surgery followed by radiation therapy to the neck.
- Radiation therapy to the mouth and the neck.
Buccal mucosa cancer
If the cancer is in the lining of the inside of the cheeks and lips (buccal
mucosa), treatment may be one of the following:
- Surgery.
- Radiation therapy.
Floor of the mouth cancer
If the cancer is in the bottom (floor) of the mouth, treatment may be one of
the following:
- Surgery.
- Radiation therapy.
Lower gum cancer
If the cancer is in the lower gums (gingiva), treatment may be one of the
following:
- Surgery.
- Radiation therapy.
Retromolar trigone cancer
If the cancer is in the small area behind the wisdom teeth, (retromolar
trigone), treatment may be one of the following:
- Surgery to remove part of the jawbone.
- Radiation therapy followed (if needed) by surgery.
Upper gums and hard palate cancer
If the cancer is in the upper gums (gingiva) or the top bony part of the
mouth (hard palate), treatment may be one of the following:
- Surgery.
- Surgery followed by radiation therapy.
Stage II Lip and Oral Cavity Cancer
Treatment depends on where the cancer is in the lip or mouth.
Lip cancer
If the cancer is in the lip, treatment may be one of the following:
- Surgery.
- External and/or internal radiation therapy.
Tongue cancer
If the cancer is in the tongue, treatment may be one of the following:
- Radiation therapy.
- Surgery and radiation therapy.
Buccal mucosa cancer
If the cancer is in the lining of the inside of the cheeks and lips (buccal
mucosa), treatment may be one of the following:
- Radiation therapy.
- Surgery.
- Surgery plus radiation therapy.
Floor of the mouth cancer
If the cancer is in the bottom (floor) of the mouth, treatment may be one of
the following:
- Surgery.
- Radiation therapy.
- Surgery followed by internal or external radiation therapy.
Lower gum cancer
If the cancer is in the lower gums (gingiva), treatment may be one of the
following:
- Surgery.
- Radiation therapy.
Retromolar trigone cancer
If the cancer is in the small space behind the wisdom teeth (retromolar
trigone), treatment may be one of the following:
- Surgery to remove part of the jawbone.
- Radiation therapy followed (if needed) by surgery.
Upper gum or hard palate cancer
If the cancer is in the upper gums or the top bony part of the mouth (hard
palate), treatment will probably be surgery followed by radiation therapy.
Stage III Lip and Oral Cavity Cancer
Treatment depends on where the cancer is in the lip or mouth. In addition to
the treatments listed below, a patient will probably have radiation therapy to
the neck with or without surgery to remove lymph nodes in the neck (lymph node
dissection).
Lip cancer
If the cancer is in the lip, treatment may be one of the following:
- Surgery to remove the cancer plus internal or external
radiation therapy.
- Radiation therapy.
- A clinical trial of chemotherapy followed by surgery or
radiation therapy.
- A clinical trial of surgery followed by chemotherapy.
- A clinical trial of surgery, radiation therapy, and
chemotherapy.
- A clinical trial of a new radiation therapy technique (superfractionated).
Tongue cancer
If the cancer is in the tongue, treatment may be one of the following:
- External beam with or without internal radiation therapy.
- Surgery followed by radiation therapy.
Buccal mucosa cancer
If the cancer is in the lining of the inside of the cheeks and lips (buccal
mucosa), treatment may be one of the following:
- Surgery to remove the cancer and the tissue around it.
- Radiation therapy.
- Surgery plus radiation therapy.
- A clinical trial of chemotherapy followed by surgery or
radiation therapy.
- A clinical trial of surgery followed by chemotherapy.
- A clinical trial of surgery, radiation therapy, and
chemotherapy.
Floor of the mouth cancer
If the cancer is in the bottom (floor) of the mouth, treatment may be one of
the following:
- Surgery to remove the cancer and lymph nodes in the neck. Part
of the jawbone may also be removed if necessary.
- External beam therapy with or without internal radiation
therapy.
- A clinical trial of chemotherapy followed by surgery or
radiation therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Lower gum cancer
If the cancer is in the lower gums (gingiva), treatment will probably be
radiation therapy given before or after surgery to remove the cancer.
Retromolar trigone cancer
If the cancer is in the small space behind the wisdom teeth (retromolar
trigone), treatment may be one of the following:
- Surgery followed by radiation therapy.
- A clinical trial of chemotherapy followed by surgery or
radiation therapy.
- A clinical trial of surgery followed by chemotherapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Upper gum or hard palate cancer
If the cancer is in the top part of the gums (gingiva) or the top bony part
of the mouth (the hard palate), treatment may be one of the following:
- Radiation therapy.
- Surgery plus radiation therapy.
For all stage III lip and oral cavity cancers, clinical trials are testing
chemotherapy combined with radiation therapy.
Stage IV Lip and Oral Cavity Cancer
Treatment depends on where the cancer is in the lip or mouth. In addition to
the treatments listed below, a patient will probably have radiation therapy to
the neck with or without surgery to remove lymph nodes in the neck (lymph node
dissection).
Lip cancer
If the cancer is in the lip, treatment may be one of the following:
- Surgery to remove the cancer plus internal or external
radiation therapy.
- A clinical trial of radiation therapy.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Tongue cancer
If the cancer is in the tongue, treatment may be one of the following:
- Surgery to remove the tongue and the voicebox (larynx) below
it followed by radiation therapy.
- Radiation therapy to relieve symptoms.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Buccal mucosa cancer
If the cancer is in the lining of the inside of the cheeks and lips (buccal
mucosa), treatment may be one of the following:
- Surgery to remove the cancer and the tissue around it.
- Radiation therapy.
- Surgery plus radiation therapy.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Floor of the mouth cancer
If the cancer is in the bottom (floor) of the mouth, treatment may be one of
the following:
- Surgery to remove the cancer followed by radiation therapy.
- Radiation therapy followed by surgery.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Lower gum cancer
If the cancer is in the lower gums (gingiva), treatment may be one of the
following:
- Surgery, radiation therapy, or both.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Retromolar trigone cancer
If the cancer is in the small space behind the wisdom teeth (retromolar
trigone), treatment may be one of the following:
- Surgery followed by radiation therapy.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Upper gum or hard palate cancer
If the cancer is in the top part of the gums (gingiva) or the top bony part
of the mouth, treatment may be one of the following:
- Surgery plus radiation therapy.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of fractionated (smaller doses) radiation
therapy.
Recurrent Lip and Oral Cavity Cancer
Treatment depends on the type of treatment the patient had before. If
radiation therapy was given, the patient may have surgery when the cancer comes
back. If surgery was used, the patient may have more surgery, radiation therapy,
or both. Patients may want to consider taking part in a clinical trial of new
chemotherapy drugs, chemotherapy plus additional radiation therapy, or
hyperthermia.
BACK
|
|
Cancer of the
oropharynx
Cancer of the oropharynx is a disease in which cancer cells are found in the
tissues of the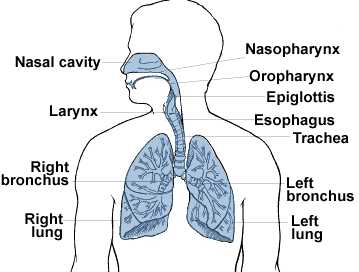 oropharynx. The oropharynx is the middle part of the throat (also
called the pharynx). The pharynx is a hollow tube about 5 inches long that
starts behind the nose and goes down to the neck to become part of the
oesophagus (tube that goes to the stomach). Air and food pass through the
pharynx on the way to the windpipe (trachea) or the oesophagus. The oropharynx
includes the soft palate (the back of the mouth), the base of the tongue, and
the tonsils. oropharynx. The oropharynx is the middle part of the throat (also
called the pharynx). The pharynx is a hollow tube about 5 inches long that
starts behind the nose and goes down to the neck to become part of the
oesophagus (tube that goes to the stomach). Air and food pass through the
pharynx on the way to the windpipe (trachea) or the oesophagus. The oropharynx
includes the soft palate (the back of the mouth), the base of the tongue, and
the tonsils.
Cancer of the oropharynx most commonly starts in the cells that line the
oropharynx. for more information on cancer that started in the lymph cells
of the oropharynx.)
A doctor should be seen if a person has a sore throat that does not go away,
trouble swallowing, a lump in the back of the mouth or throat, a change in the
voice, or pain in the ear.
If there are symptoms, a doctor will examine the throat using a mirror and
lights. The doctor will also feel the throat for lumps. If tissue that is not
normal is found, the doctor will need to cut out a small piece and look at it
under the microscope to see if there are any cancer cells. This is called a
biopsy.
The chance of recovery (prognosis) depends on where the cancer is in the
throat, whether the cancer is just in the throat or has spread to other tissues
(the stage), and the patient’s general state of health. After the treatment, a
doctor should be seen regularly because there is a chance of having a second
cancer in the head or neck region.
Stages of cancer of the oropharynx
Once cancer of the oropharynx is found, more tests will be done to find out
if cancer cells have spread to other parts of the body. This is called staging.
A doctor needs to know the stage of the disease to plan treatment. The following
stages are used for cancer of the oropharynx.
Stage I
The cancer is no more than 2 centimetres (about 1 inch) and has not spread to
lymph nodes in the area (lymph nodes are small bean-shaped structures that are
found throughout the body; they produce and store infection-fighting cells).
Stage II
The cancer is more than 2 centimetres, but less than 4 centimetres (less than
2 inches), and has not spread to lymph nodes in the area.
Stage III
Either of the following may be true:
- The cancer is more than 4 centimetres.
- The cancer is any size but has spread to only one lymph node
on the same side of the neck as the cancer. The lymph node that contains
cancer measures no more than 3 centimetres (just over one inch).
Stage IV
Any of the following may be true:
- The cancer has spread to tissues around the oropharynx. The
lymph nodes in the area may or may not contain cancer.
- The cancer is any size and has spread to more than one lymph
node on the same side of the neck as the cancer, to lymph nodes on one or both
sides of the neck, or to any lymph node that measures more than 6 centimetres
(over 2 inches).
- The cancer has spread to other parts of the body.
Recurrent
Recurrent disease means that the cancer has come back (recurred) after it has
been treated. It may come back in the oropharynx or in another part of the body.
How cancer of the oropharynx is treated
There are treatments for all patients with cancer of the oropharynx. Three
kinds of treatment are used:
- Surgery (taking out the cancer).
- Radiation therapy (using high-dose x-rays or other high-energy
rays to kill cancer cells).
- Chemotherapy (using drugs to kill cancer cells).
Hyperthermia (warming the body to kill cancer cells) is being tested in
clinical trials.
Surgery is a common treatment of cancer of the oropharynx. A doctor may
remove the cancer and some of the healthy tissue around the cancer. If cancer
has spread to lymph nodes, the lymph nodes will be removed (lymph node
dissection). A new type of surgery called micrographic surgery is being tested
in clinical trials for early cancers of the oropharynx. Micrographic surgery
removes the cancer and as little normal tissue as possible. During this surgery,
the doctor removes the cancer and then uses a microscope to look at the
cancerous area to make sure there are no cancer cells remaining.
Radiation therapy uses high-energy x-rays to kill cancer cells and shrink
tumours. Radiation may come from a machine outside the body (external radiation
therapy) or from putting materials that produce radiation (radioisotopes)
through thin plastic tubes in the area where the cancer cells are found
(internal radiation therapy). External radiation to the thyroid or the pituitary
gland may change the way the thyroid gland works. The doctor may wish to test
the thyroid gland before and after therapy to make sure it is working properly.
Giving drugs with the radiation therapy to make the cancer cells more sensitive
to radiation (radiosensitization) is being tested in clinical trials. If smoking
is stopped before radiation therapy is started, there is a better chance of
surviving longer.
Chemotherapy uses drugs to kill cancer cells. Chemotherapy may be taken by
pill, or it may be put into the body by a needle in the vein or muscle.
Chemotherapy is called a systemic treatment because the drug enters the
bloodstream, travels through the body, and can kill cancer cells throughout the
body.
People with oropharyngeal cancer have a higher risk of getting other cancers
in the head and neck area. Clinical trials of chemoprevention therapy are
testing whether certain drugs can prevent second cancers from developing in the
mouth, throat, windpipe, nose, or oesophagus (the tube that connects the throat
to the stomach).
Hyperthermia uses a special machine to heat the body for a certain period of
time to kill cancer cells. Because cancer cells are often more sensitive to heat
than normal cells, the cancer cells die and the cancer shrinks.
Because the oropharynx helps in breathing, eating, and talking, patients may
need special help adjusting to the side effects of the cancer and its treatment.
A doctor will consult with several kinds of doctors who can help determine the
best treatment. Trained medical staff can also help patients recover from
treatment and adjust to new ways of eating and talking. Plastic surgery, or help
learning to eat and speak, may be needed if a large part of the oropharynx is
taken out.
Stage I Oropharyngeal Cancer
Treatment will be surgery to remove the cancer or radiation therapy
Stage II Oropharyngeal Cancer
Treatment will be surgery to remove the cancer or radiation therapy
Stage III Oropharyngeal Cancer
Treatment may be one of the following:
- Surgery to remove the cancer followed by radiation therapy.
- Radiation therapy.
- A clinical trial of chemotherapy followed by surgery or
radiation therapy.
- A clinical trial of chemotherapy combined with radiation
therapy.
- A clinical trial of new ways of giving radiation therapy.
Stage IV Oropharyngeal Cancer
If the cancer can be removed by surgery, treatment may be one of the
following:
- Surgery to remove the cancer followed by radiation therapy.
- Radiation therapy.
- A clinical trial of radiation therapy combined with
chemotherapy.
- A clinical trial of new ways of giving radiation therapy.
If the cancer cannot be removed by surgery, treatment may be one of the
following:
- Radiation therapy. Clinical trials are testing new ways of
giving radiation therapy.
- A clinical trial of chemotherapy followed by surgery or
radiation therapy.
- A clinical trial of radiation therapy given with chemotherapy
or with drugs to make the cancer cells more sensitive to radiation therapy (radiosensitizers).
- A clinical trial of hyperthermia plus radiation therapy.
Recurrent Oropharyngeal Cancer
Treatment may be one of the following:
- Surgery to remove the cancer.
- Radiation therapy.
- A clinical trial of chemotherapy.
- A clinical trial of hyperthermia plus radiation therapy.
BACK
|


 the neck that lasts more than two weeks should be
seen by a doctor as soon as possible. Of course, not all lumps are cancer.
But a lump (or lumps) in the neck can be the first sign of cancer of the
mouth, throat, voicebox (larynx), thyroid gland, or of certain lymphomas
or blood cancers. Such lumps are generally painless and continue to
enlarge steadily.
the neck that lasts more than two weeks should be
seen by a doctor as soon as possible. Of course, not all lumps are cancer.
But a lump (or lumps) in the neck can be the first sign of cancer of the
mouth, throat, voicebox (larynx), thyroid gland, or of certain lymphomas
or blood cancers. Such lumps are generally painless and continue to
enlarge steadily.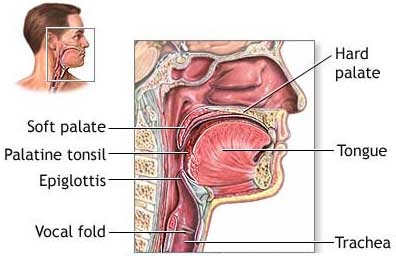
 Many patients also need swallowing therapy after treatment to help them adjust
to the changes in their throat. Throat cancers can be cured in 90% of patients
if detected early. If the cancer has spread to surrounding tissues or lymph
nodes in the neck 50-60% of patients can be cured. If the cancer has spread
(metastasized) to parts of the body outside the head and neck, the cancer is not
curable and treatment is aimed at prolonging quality of life.
Many patients also need swallowing therapy after treatment to help them adjust
to the changes in their throat. Throat cancers can be cured in 90% of patients
if detected early. If the cancer has spread to surrounding tissues or lymph
nodes in the neck 50-60% of patients can be cured. If the cancer has spread
(metastasized) to parts of the body outside the head and neck, the cancer is not
curable and treatment is aimed at prolonging quality of life.